

FDA has Gone Rogue
Paraphrasing Dr. Peter Marks: "We don' need no public health emergency to emergency use authorize mismatched boosters"

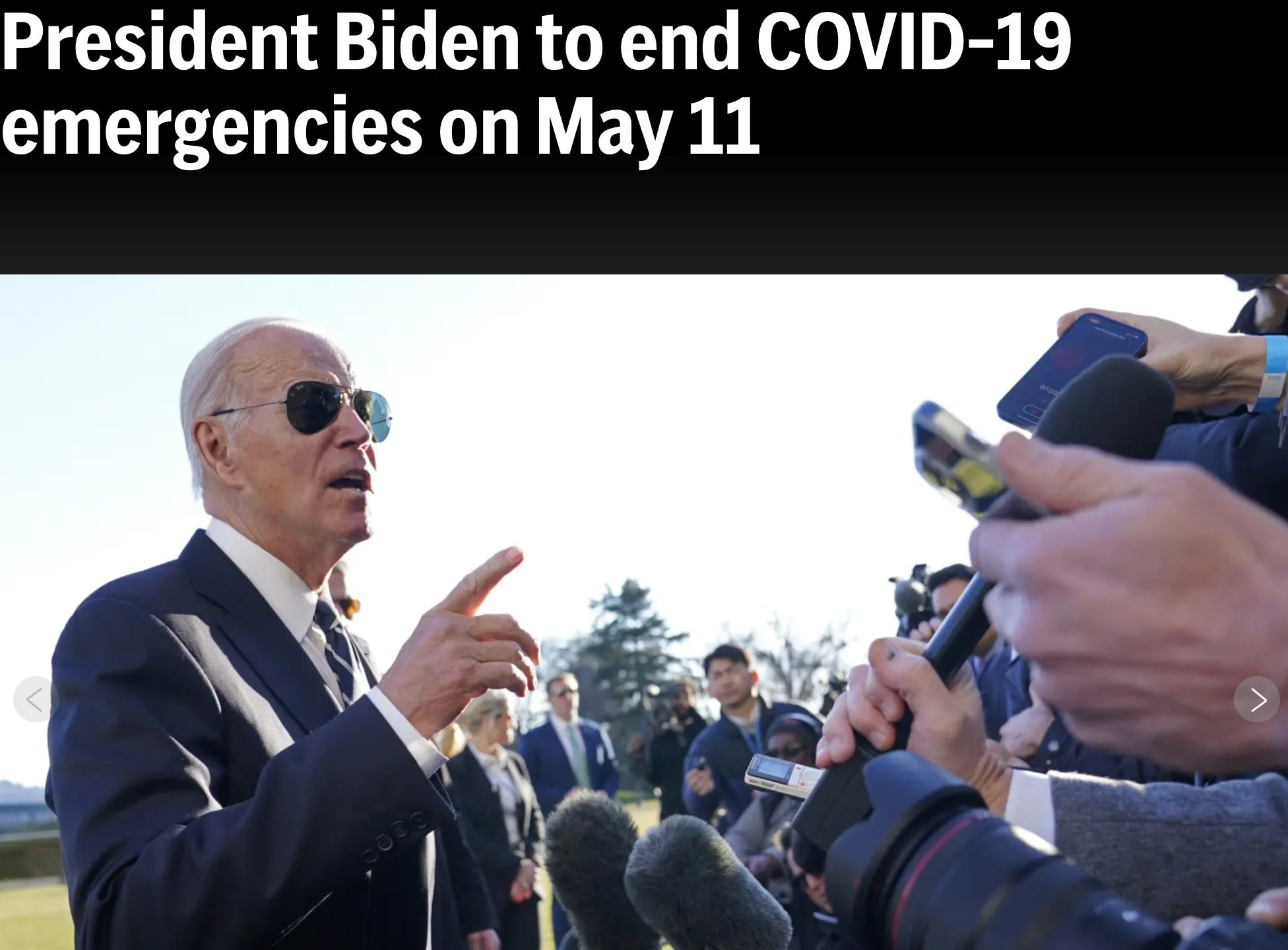
President Biden to end COVID-19 emergencies on May 11
Associated Press, January 30, 2023
WASHINGTON (AP) — President Joe Biden informed Congress on Monday that he will end the twin national emergencies for addressing COVID-19 on May 11, as most of the world has returned closer to normalcy nearly three years after they were first declared.
The move to end the national emergency and public health emergency declarations would formally restructure the federal coronavirus response to treat the virus as an endemic threat to public health that can be managed through agencies’ normal authorities.
It comes as lawmakers have already ended elements of the emergencies that kept millions of Americans insured during the pandemic. Combined with the drawdown of most federal COVID-19 relief money, it would also shift the development of vaccines and treatments away from the direct management of the federal government.
Biden’s announcement comes in a statement opposing resolutions being brought to the floor this week by House Republicans to bring the emergency to an immediate end. House Republicans are also gearing up to launch investigations on the federal government’s response to COVID-19.
Many of us knew this day would come, and now here it is. As of Monday, September 11, 2023, the FDA has provided “Emergency Use Authorization” for the SARS-CoV-2 mRNA vaccine boosters. But there is no public health emergency at this time. And the “boosters” being “Emergency Use Authorized” are designed to provide protection against the Omicron variant called “Kraken”. Which is on its way to becoming extinct, outcompeted by newer variants like Eris which have evolved even further to escape the antibody pressure elicited by the globally deployed leaky “vaccines”.
Prior versions of which boosters, by the way, have been shown to have been adulterated with high levels of plasmid DNA incorporating SV40 virus promoter/enhancer sequences. Which adulteration the FDA continues to ignore.
“Vaccination remains critical to public health and continued protection against serious consequences of COVID-19, including hospitalization and death,” said Peter Marks, M.D., Ph.D., director of the FDA’s Center for Biologics Evaluation and Research. “The public can be assured that these updated vaccines have met the agency’s rigorous scientific standards for safety, effectiveness, and manufacturing quality. We very much encourage those who are eligible to consider getting vaccinated.”
But Biden, under congressional pressure, had decided and certified that the COVIDcrisis “national emergency” ended May 11, 2023, right? Sort of.
The administrative class at the FDA decided that they have the authority to interpret this in their own special way. Despite clear Congressional intent and the Presidential decision, the FDA responded with a series of delaying tactics. These are summarized in an “action notice” in the Federal Register titled “Guidance Documents Related to Coronavirus Disease 2019 (COVID-19), A Notice by the Food and Drug Administration on 03/13/2023”. At the time of the Presidential declaration, the FDA had 72 COVID-19-related guidance documents currently in effect. These are not law, they are administrative guidance, but often function and are enforced as if they are law. If you are seeking an example of administrative state overreach, this would be a good place to start. So, whats an agency to do? Issue an action notice in the federal register laying out new rules, functionally a guidance on guidances.
So here are the new rules, as unilaterally determined by FDA administrators. They took those 72 COVID-19 related guidances and divided them into four tables, and determined what they would mandate for the guidances in each table.
Table 1 were those that would expire when the public health emergency (PHE) would expire.
Table 2 were those that would be revised to continue in effect for 180 days after the PHE declaration expires, then will no longer be in effect on November 07, 2023 (Tuesday).
Table 3 were those to be revised to continue in effect for 180 days after the PHE declaration expires, during which time FDA plans to further revise these guidances <and then ??>.
Table 4 lists COVID-19-related guidance documents whose intended duration is not tied to the COVID-19 PHE and that will remain in effect when the COVID-19 PHE declaration expires. In other words, by administrative fiat, those guidances listed in Table 4 will remain in place for as long as the FDA administrators wish them to remain in place.
And at the top of Table 3 (the ones that they will revise as they see fit and continue as long as they think necessary) is the following:
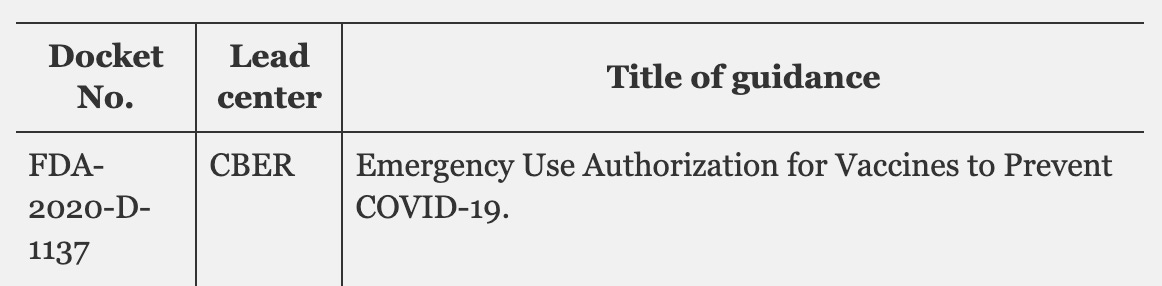
Did they actually revise FDA-2020-D-1137 between then and now? Did they do the work that they said they would do? In short, no. The guidance remains unrevised since March 2022.
What congressional law and language determines when FDA can issue EUAs?
From the FDA’s own website regarding Emergency Use Authorization-
Under section 564 of the Federal Food, Drug, and Cosmetic Act (FD&C Act), when the Secretary of HHS declares that an emergency use authorization is appropriate, FDA may authorize unapproved medical products or unapproved uses of approved medical products to be used in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by CBRN threat agents when certain criteria are met, including there are no adequate, approved, and available alternatives.
So, basically, the FDA administrative bureaucracy self-determined that they could continue to bypass their normal (already lax) procedures for evaluating vaccine purity (including lack of adulteration), potency, safety and efficacy pretty much for as long as their hearts desire, at least until November 07, 2023. And that is the administrative basis used to enable the September 11, 2023 “Emergency Use Authorization” for the SARS-CoV-2 mRNA vaccine boosters. Will that authorization sunset on November 07, 2023? I very much doubt it.
Meanwhile, back at the capital dome, the leadership of the congressional gerontocracy continued to snooze, raise funds for the next election, and almost daily demonstrate to the world (during rare public appearances) their quite literal mental incompetence (in a strict medical sense of the term).
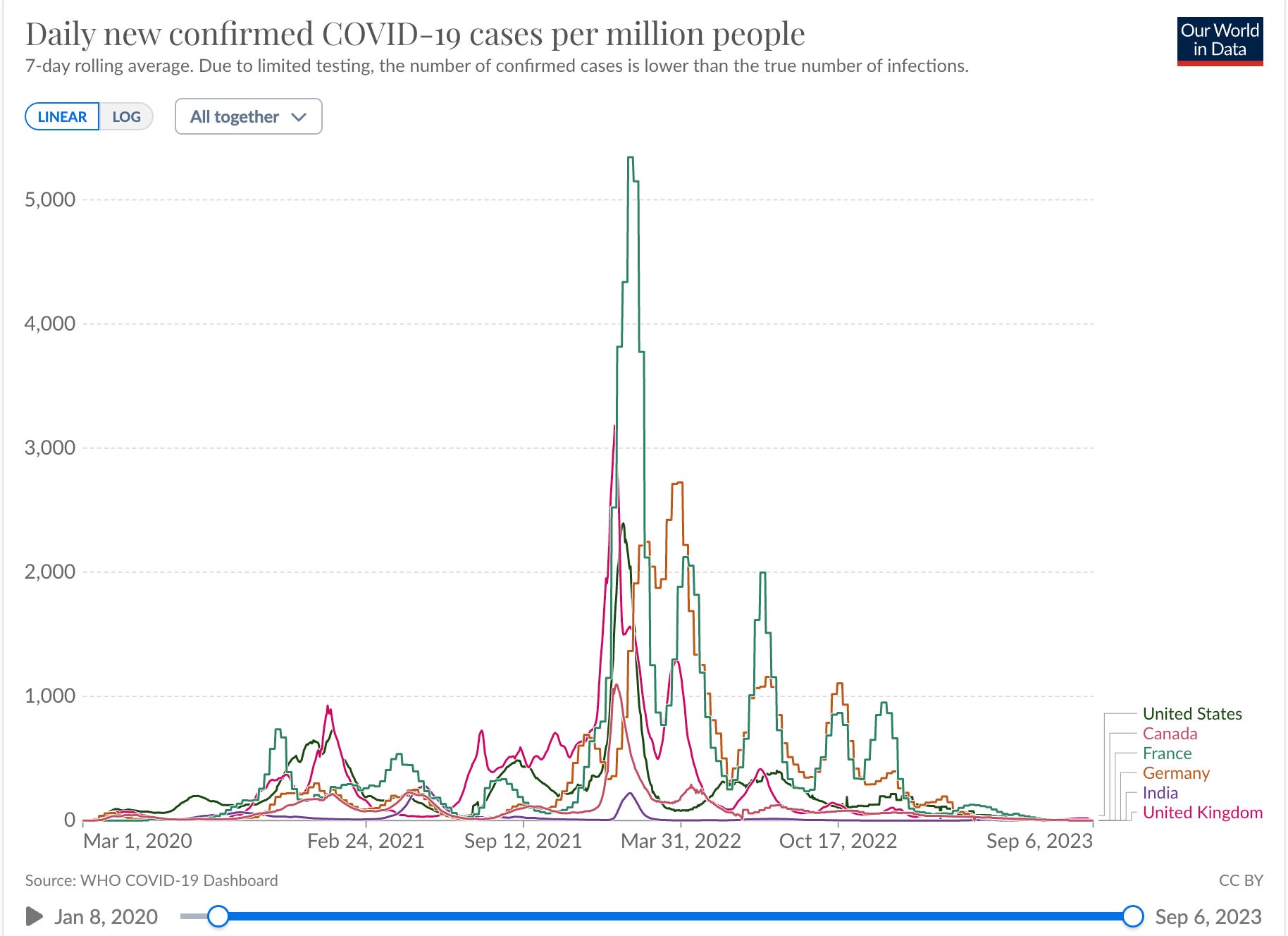
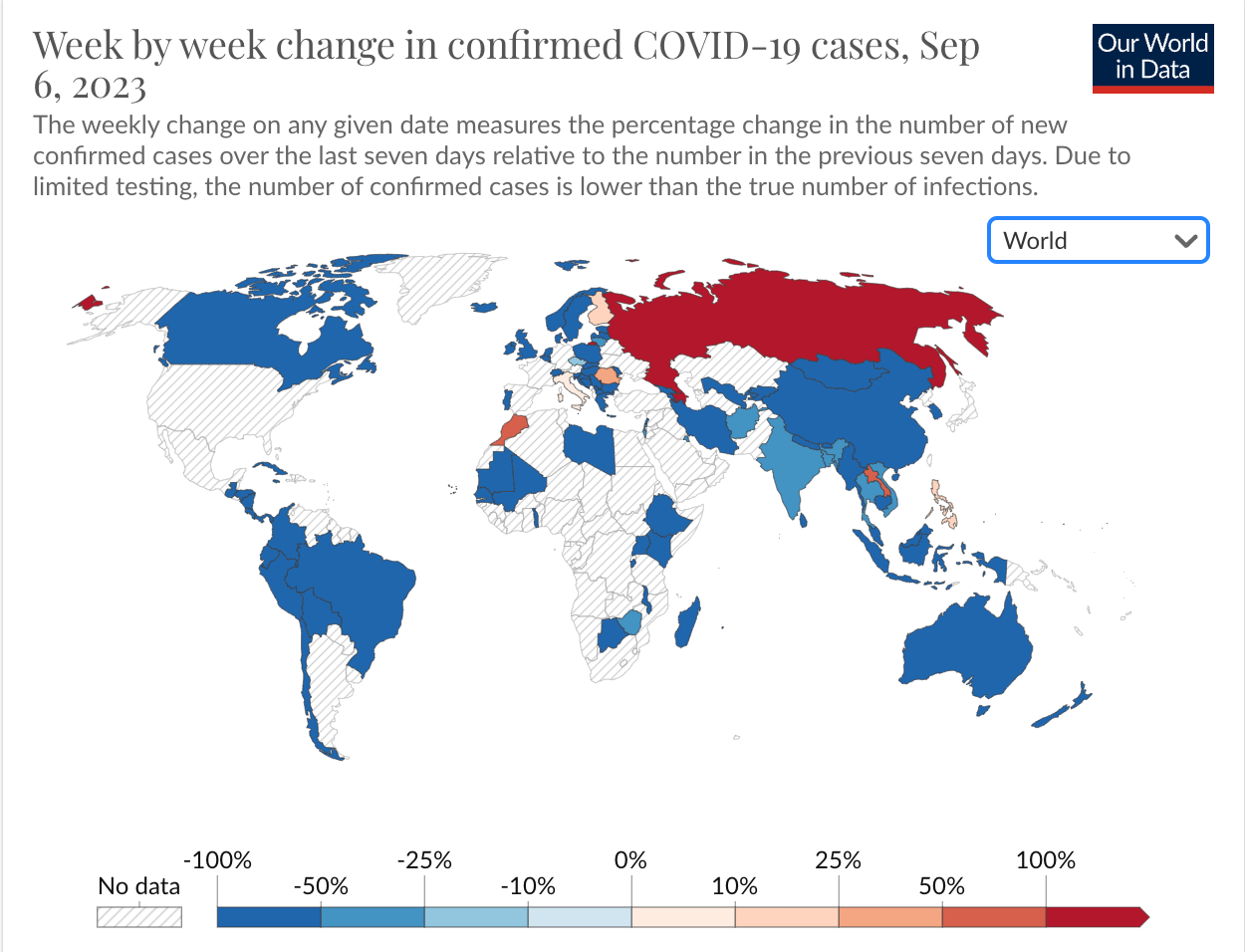
The data clearly demonstrate that there is no longer a COVID public health emergency, and there are no human data demonstrating safety and effectiveness of these mismatched “vaccine booster” products.
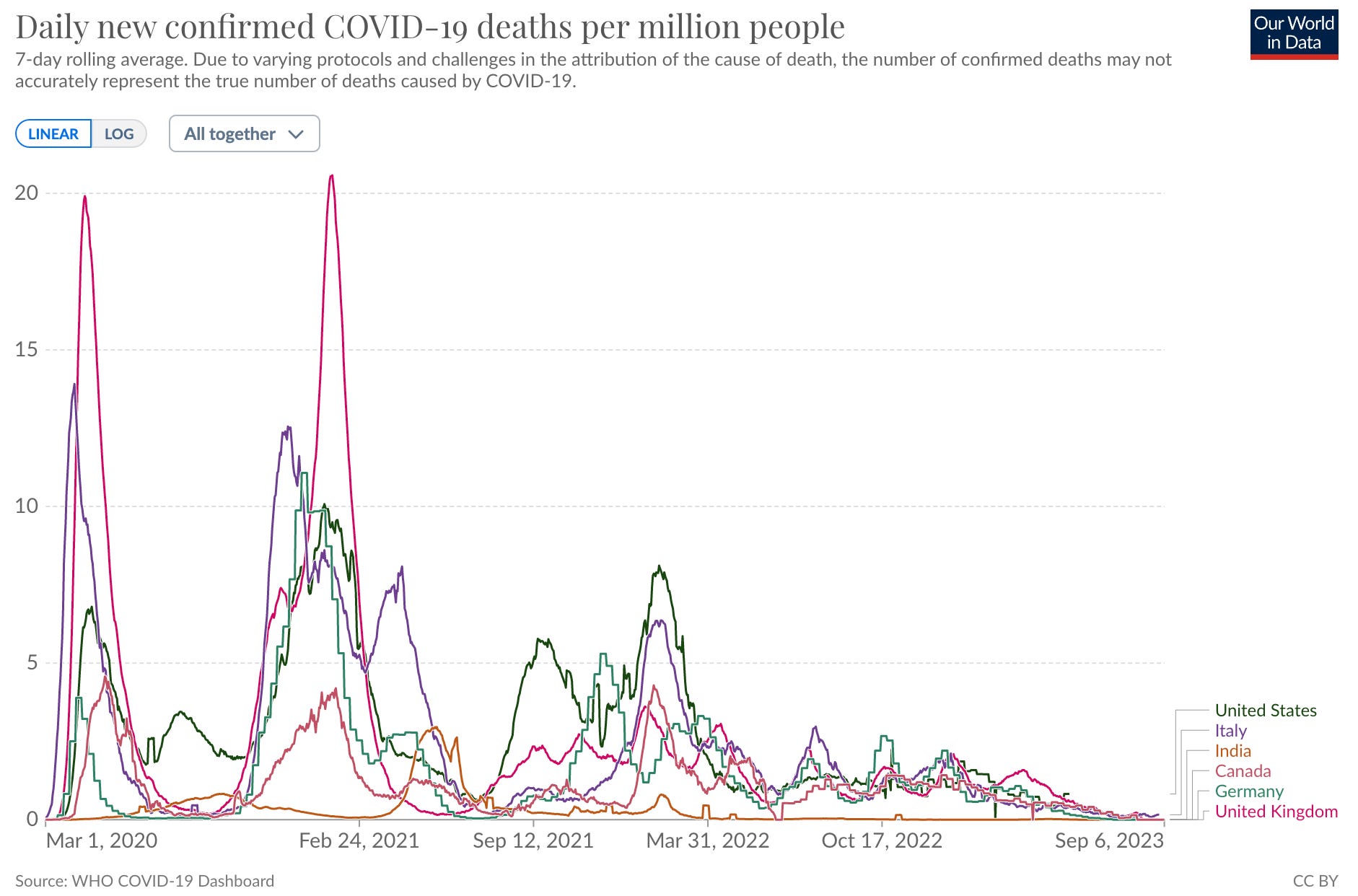
World data:
What do the current CDC data show in the USA (total deaths)?
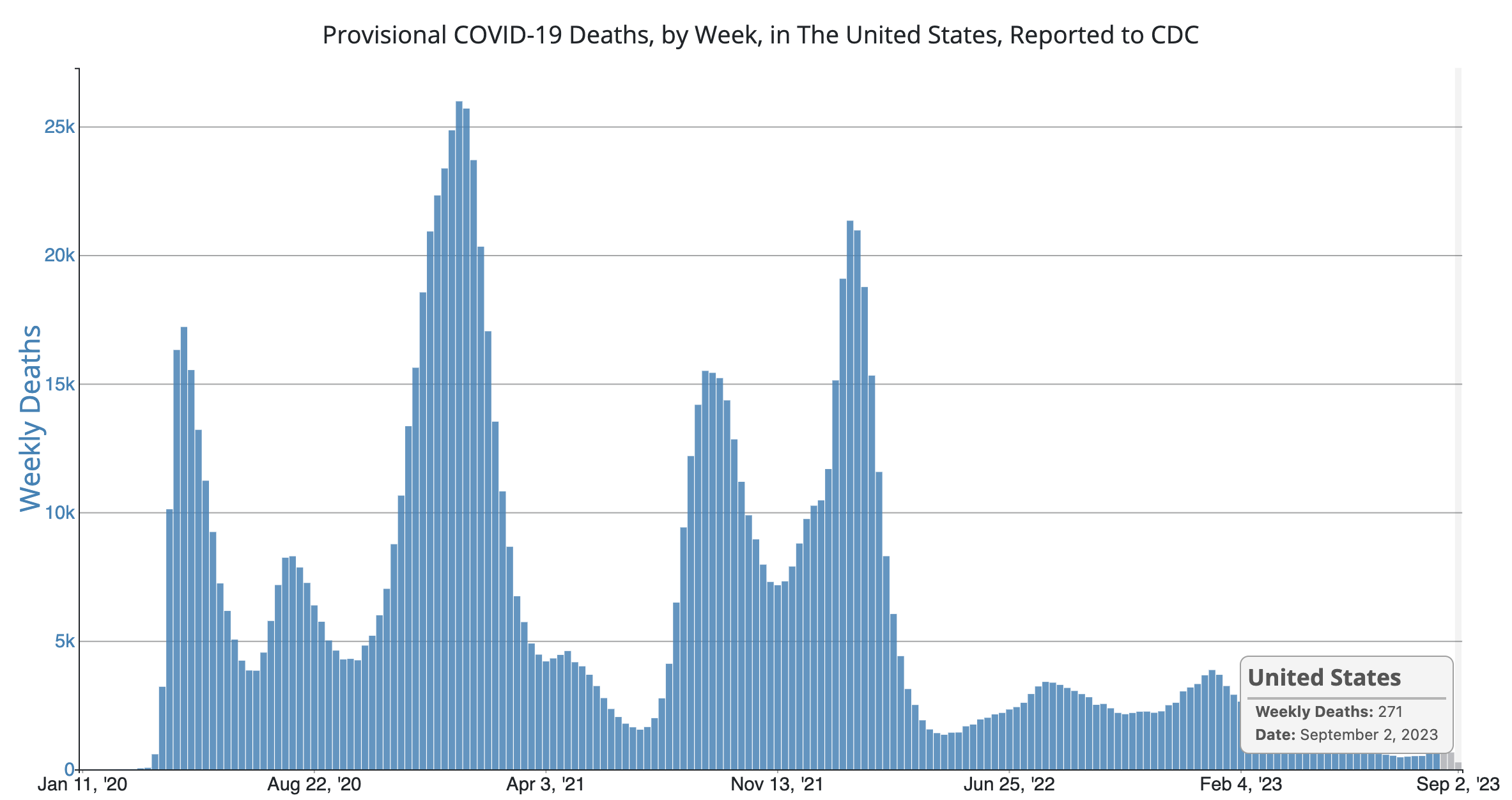
271 deaths per week, 38 deaths per day WITH COVID. In contrast, we loose 200 - 300 mostly young people per day to Fentanyl and other opiates. That is 1400 deaths per week from drug overdoses. As if one 737 full of young US citizens crashed and killed all passengers per week. Five times the COVID deaths. If opioid deaths are not a public health emergency, then why is COVID an emergency?
The obvious answer is that it is not.
Hospitalization data:
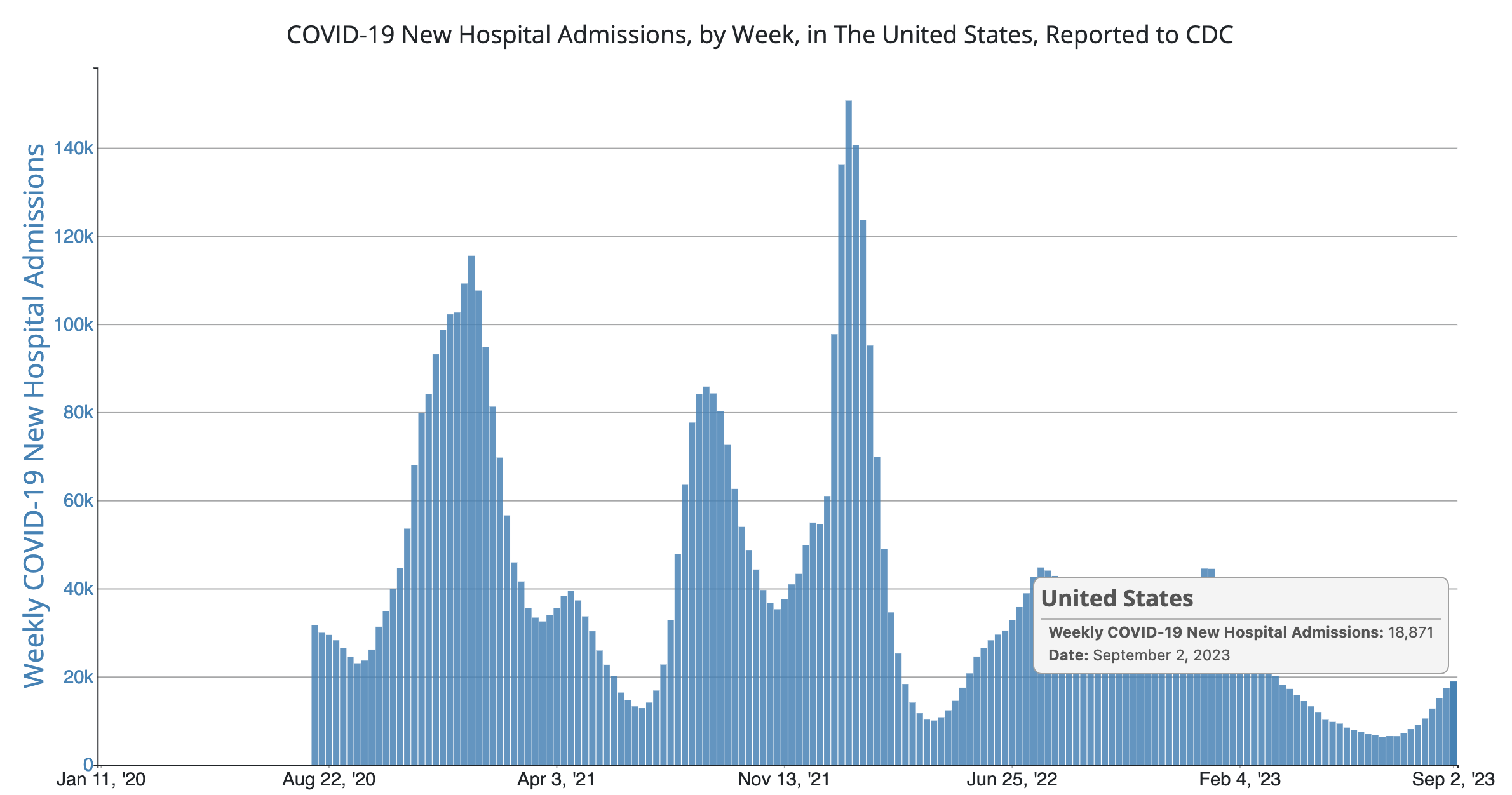
Hospitalized cases are up in the USA. But deaths are down. Not surprising, as the majority of currently circulating SARS-CoV-2 virus are more highly evolved Omicron variants. Typically more infectious, less pathogenic, and better adapted to evade the narrow antibody-based anti-Spike immune responses elicited by these leaky vaccines.
Who are the ones that are being hospitalized? More of them are the ones that have received a Moderna or Pfizer Emergency Use Authorized mRNA “vaccine” product than have not. That is a fact long known by the US Government, but hidden until internal government discussions about this were recently documented by FOIA request.
I infer that the real crisis here is that the data from all over the world are clearly demonstrating that some period of time after receiving a mRNA “Booster vaccine”, recipients are developing “negative effectiveness”.
What the heck is “negative effectiveness”, you may well ask? The term means that those who have received the product are more likely to develop COVID than those who have not been injected. And there are suggestions in the data that the period of time between injection and “negative effectiveness” is getting shorter.
Even if the “vaccine” products even have zero rather than negative effectiveness, they certainly have toxicity risks, so why would anyone be willing to receive these products if they knew this?
The “vaccinated” are at higher risk for developing COVID than the unvaccinated. So the “vaccinated” need more “vaccines”. So they can become at yet higher risk for COVID (and other infectious diseases)? Somehow the Joseph Heller WW-II book “Catch-22” comes to mind.
And why would the FDA provide “emergency use authorization” and the CDC recommend these clearly toxic products for children?


While speaking at a Thursday news conference for Gov. Ron DeSantis in Jacksonville, Florida, Dr. Joseph Ladapo, that state's surgeon general, advised people to steer clear of the updated booster vaccine for COVID-19.
The U.S. Food and Drug Administration (FDA) has not yet approved the new vaccine — which is reportedly designed to protect against the BA.2.86 omicron subvariant.
"There’s a new vaccine that’s coming around the corner, a new mRNA COVID-19 vaccine, and there’s essentially no evidence for it," Ladapo said during the news conference, according to local news outlets.
"There’s been no clinical trial done in human beings showing that it benefits people" he said.
"There’s been no clinical trial showing that it is a safe product for people — and not only that, but then there are a lot of red flags."
In terms of specific concerns, Ladapo warned that the updated vaccines "actually cause cardiac injury in many people."
The state surgeon general urged Floridians to make their own decisions based on their particular "resonance of truth," rather than on "very educated people telling you what you should think."
"When they try to convince you to be comfortable and agree with things that don’t feel comfortable, [that] don’t feel like things you should agree with, that is a sign, right? That’s a gift," he said.
Instead of relying on the new vaccines, Ladapo urged people to adopt healthy nutrition habits.
Just for the record, I completely agree with Dr. Ladipo. But I also recommend checking your vitamin D levels, and taking vitamin D together with Zinc supplements in alignment with your personal physician’s recommendations. And get outside. And don’t forget that stress and fear are immunosuppressive.
Maybe you should think about following John Prine’s advice and blow up your TV. The fearporn being promoted on television and corporate media is hazardous to both your health and your ability to make rational health decisions for yourself and your family.
Lets discuss the data which the FDA cites. Here is their statement:
The mRNA COVID-19 vaccines approved and authorized today are supported by the FDA’s evaluation of manufacturing data to support the change to the 2023-2024 formula and non-clinical immune response data on the updated formulations including the XBB.1.5 component.
OK, what does that mean? Non-clinical immune response data? What it means is that they administered the XBB.1.5 (that would be Kraken) variant vaccine products to mice, drew blood, and tested the mouse antibody responses to the XBB.1.5 as well as EG.5 (Eris) and BA.2.86 (that would be Pirola, previously discussed here) viral variants to see if the mouse serum would stop the ability of these viruses to infect cultured cells. Neither of which viral variants (XBB.1.5, EG.5, or BA.2.86) present much of a health risk. And they assert that they found that the mouse antibodies cross reacted against Eris and Pirola in a virus neutralization test. But they did not bother to share those data with the public, so we have no idea of how convincing or even how rigorously controlled those studies were. But we are to trust that the FDA finds these studies involving mouse model testing using a method that has not been demonstrated to predict protection against infection, replication, or spread of this virus in humans. But which the corporate media thinks sounds very sciency and so they breathlessly repeat the FDA and Pfizer statements about mouse neutralization assays as if they demonstrate that these “boosters” will be effective. But it is all a lie, a sleight of hand. This is not how modern immunological science is done. This is propaganda and marketing. And the willingness of FDA to make the above statement clearly demonstrates that they are either 1) completely incompetent, 2) barking mad, or 3) completely captured. Or come combination of all three.
Note that nothing in the FDA justification addresses the risk to human health posed by these viral variants. The FDA has completely avoided any justification for the use of the emergency use authorization pathway, rather than a more standard, traditional testing and evaluation process. Because they do not think that they need to. This provides yet another example of the arrogance of the current administrative leviathan.
Once again- VIRUS NEUTRALIZATION IS NOT A PROVEN CORRELATE OF PROTECTION. Back in the day, before 2020, if a vaccine company were so bold as to assert that a mouse virus neutralization assay (or any other lab test) predicted vaccine protection in humans without having proven that the assay actually predicted whether or not the vaccine would protect humans, they would be sued and blocked from making such false unsupported claims. But since 2020, this type of claim has become routine. The FDA has gone completely rogue. They completely disregard what was previously well established global regulatory standards on this subject.
The updated mRNA vaccines are manufactured using a similar process as previous formulations. In studies that have been recently conducted, the extent of neutralization observed by the updated vaccines against currently circulating viral variants causing COVID-19, including EG.5 and BA.2.86, appears to be of a similar magnitude to the extent of neutralization observed with prior versions of the vaccines against corresponding prior variants against which they had been developed to provide protection. This suggests that the vaccines are a good match for protecting against the currently circulating COVID-19 variants.
Lies and falsehoods on top of lies and falsehoods. There is clear evidence that the manufacturing process is poorly controlled, lots are highly variable, and this poorly controlled process has resulted in significant adulteration of the products.
Furthermore, mouse-based viral neutralization assays do not predict effectiveness in “protecting against the currently circulating COVID-19 variants”. There is no evidence to support that claim. This is yet another case of substituting hope for actual scientific proof. There is no evidence that these mismatched boosters will prevent infection, replication, or spread of currently circulating COVID-19 variants. A “suggestion” is not a rational basis for “Emergency Use” regulatory authorization of these products.
The benefit-risk profile of previously authorized and approved mRNA COVID-19 vaccines is well understood as these vaccines have been administered to hundreds of millions of people in the United States.
That is a highly controversial statement. I disagree, Dr. Joe Ladipo disagrees, and regulatory oversight agencies from an increasing number of countries all over the world disagree. Just because the government and manufactures have colluded to force hundreds of millions of people to accept these products (without informed consent) does not prove anything. Repeatedly stating a lie does not make it true. This is clearly propaganda.
The data demonstrate otherwise. The benefit-risk ratio is upside down. Little or no benefit, many well documented risks. And immune imprinting. And negative effectiveness. And they DO NOT PREVENT infection, replication, and transmission of the virus to others. Herd immunity can never be achieved with these leaky vaccines. That was yet another Fauci (and Biden) lie.
And then there are the many analytical flaws in the cited data analyses. Which always seem to be biased in favor of vaccine effectiveness. For a deep dive into that, I recommend the following:
“The imprinting effect of covid-19 vaccines: an expected selection bias in observational studies” (Response)
BMJ2023;381doi:https://doi.org/10.1136/bmj-2022-074404(Published 07 June 2023)Cite this as:BMJ2023;381:e074404 (article)
We need proper explanations for apparent COVID-19 vaccine negative effectiveness
Dear Editor
A striking phenomenon regarding COVID-19 vaccines, referred to as ‘immune imprinting’ or the more specific ‘negative effectiveness’, has been recently discussed here in The BMJ.1 Referring to Chemaitelly et al., which indicated that those with 3 doses of vaccine were more likely to be infected than those with 2, 2 Monge et al. hypothesise that “the increased risk of reinfection in individuals vaccinated with a booster compared with no booster is the result” of a selection bias wherein those receiving the booster are those “more susceptible to reinfection”; a sort of counter to the hypothesised ‘healthy vaccinee bias’. Apart from the article’s inconclusive conclusion that this phenomenon “may be fully explained by selection bias”, this hypothesis would not apply to all such studies.
For example, while it could be reasonable to suppose that people opting for dose 3 and beyond would tend to be at higher risk of COVID-19, and thus more prone to reinfection, it is not obvious that this would apply to the recent study on healthcare workers presented by Shrestha et al.3 This study reveals an even greater problem. The phenomenon is not limited to boosters but is also found when comparing those receiving 2 doses to those receiving 0. In fact, Shrestha et al. indicates that each dose up to 3+ resulted in increased infections. And there are many other studies showing this phenomenon, also with regards to hospitalisations and deaths, in addition to the now widely accepted rapid waning of effectiveness, when comparing the double dosed to the unvaccinated, including another study with Chemaitelly as lead author.4 5 Several recently published papers also explain how counting window issues likely led to exaggerated effectiveness and safety estimates in both observational studies and clinical trials.6 7 8
The explanation offered up by Monge et al. fails. What we need is a proper explanation for perceived COVID-19 vaccine negative effectiveness, by the vaccine manufacturers or drug regulators. We need to know if this has always been the case or only since omicron, if the effect is dose-dependent, if certain groups are more at risk, etc. Otherwise, the notion that the benefits of the COVID-19 vaccines outweighs the risks is under threat. If the vaccines truly are negatively effective, it appears that the benefits do not outweigh the risks; there would be no benefits, and we simply add risks upon risks.
References
1. Monge S, Pastor-Barriuso R, Hernán MA. The imprinting effect of covid-19 vaccines: an expected selection bias in observational studies. BMJ. 2023;381:e074404. https://doi.org/10.1136/bmj-2022-074404.
2. Chemaitelly H, Ayoub HH, Tang P, et al. Long-term COVID-19 booster effectiveness by infection history and clinical vulnerability and immune imprinting: a retrospective population-based cohort study. The Lancet Infectious Diseases. 2023;23:816-27. https://doi.org/10.1016/S1473-3099(23)00058-0.
3. Shrestha NK, Burke PC, Nowacki AS, et al. Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine. Open Forum Infectious Diseases. 2023;10:ofad209. https://doi.org/10.1093/ofid/ofad209.
4. Goldberg Y, Mandel M, Bar-On YM, et al. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. New England Journal of Medicine. 2022;386:2201-12. https://www.nejm.org/doi/full/10.1056/NEJMoa2118946.
5. Chemaitelly H, Ayoub H, AlMukdad S, et al. Protection from previous natural infection compared with mRNA vaccination against SARS-CoV-2 infection and severe COVID-19 in Qatar: a retrospective cohort study. The Lancet Microbe. 2022;3:e944-55. https://doi.org/10.1016/S2666-5247(22)00287-7.
6. Fung K, Jones M, Doshi P. Sources of bias in observational studies of covid-19 vaccine effectiveness. Journal of Evaluation in Clinical Practice. 2023;1-7. https://doi.org/10.1111/jep.13839.
7. Lataster R. Reply to Fung et al. on COVID-19 vaccine case-counting window biases overstating vaccine effectiveness. Journal of Evaluation in Clinical Practice. 2023;1-4. https://doi.org/10.1111/jep.13892.
8. Doshi P, Fung K. How the case counting window affected vaccine efficacy calculations in randomized trials of COVID-19 vaccines. Journal of Evaluation in Clinical Practice. 2023;1-2. https://doi.org/10.1111/jep.13900.
“Long-term COVID-19 booster effectiveness by infection history and clinical vulnerability and immune imprinting: a retrospective population-based cohort study”
Lancet Infectious Diseases VOLUME 23, ISSUE 7, P816-827, JULY 2023
In the seventh month and thereafter, coincident with BA.4/BA.5 and BA.2·75* subvariant incidence, effectiveness was progressively negative albeit with wide CIs. Similar patterns of protection were observed irrespective of previous infection status, clinical vulnerability, or type of vaccine (BNT162b2 vs mRNA-1273).
Interpretation
Protection against omicron infection waned after the booster, and eventually suggested a possibility for negative immune imprinting.
Interpretation
Protection against omicron infection waned after the booster, and eventually suggested a possibility for negative immune imprinting. However, boosters substantially reduced infection and severe COVID-19, particularly among individuals who were clinically vulnerable, affirming the public health value of booster vaccination.

Sources of bias in observational studies of covid-19 vaccine effectiveness
Kaiser Fung MPhil, MBA, Mark Jones PhD, Peter Doshi PhD
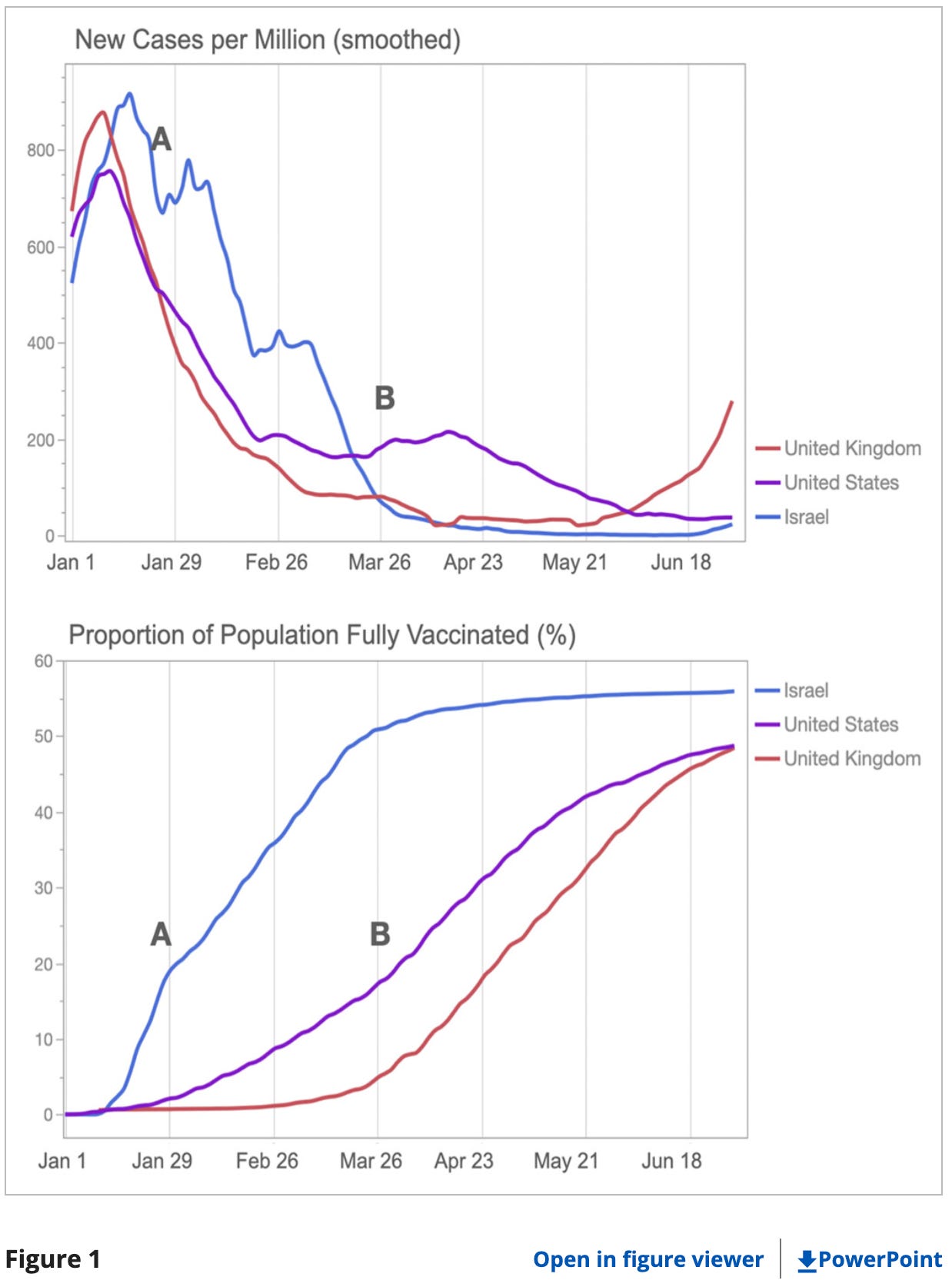
In late 2020, messenger RNA (mRNA) covid-19 vaccines gained emergency authorisation on the back of clinical trials reporting vaccine efficacy of around 95%,1, 2 kicking off mass vaccination campaigns around the world. Within 6 months, observational studies reporting vaccine effectiveness in the “real world” at above 90%, similar to trial results,3-6 became the trusted source of evidence upholding these campaigns. While the contemporary conversation about vaccine effectiveness has turned to waning protection, virus variants, and boosters, there has (with rare exception7) been surprisingly little discussion of the limitations of the methodologies of these early observational studies.
The lack of critical discussion is notable, for even highly effective vaccinations could only partially explain the drop in rates of covid-19 cases, hospitalisations, and deaths by mid-2021. For example, by March 2021, cases in the UK and United States had dropped roughly fourfold from the January peak, when the “fully vaccinated” population only reached 20% and 5%, respectively. At the same time, in Israel, cases took longer to drop despite a substantially faster vaccine rollout (Figure 1). The vaccination campaigns in these countries can thus only be part of the story.
"There’s been no clinical trial done in human beings showing that it benefits people… There’s been no clinical trial showing that it is a safe product for people — and not only that, but then there are a lot of red flags."
-Surgeon General of Florida, Dr. Joe Ladapo
“Who is Robert Malone” is a reader supported publication, please consider becoming a subscriber.
At this point, the whole damn government has gone rogue and is now a pure mafia-like cabal-ruled organization.
Should be crystal clear anyone breathing that the government is owned by BigPharma and the military- industrial complex