



Honey, Why Do Viral Outbreaks Happen In Children Every Few Years?
It's complicated, but also surprisingly simple.

Did you ever wonder why outbreaks of viral diseases seem to happen in occasional (geographically based) waves of infection? And why do these viral waves tend to periodically circle the world?
How about why an outbreak will start, grow, taper off, and then re-emerge a few years later? Whether or not “public health” intervenes?
A natural process has been going on for as long as viruses have been interacting with humans and other animals with immune systems that can adapt to fight different viruses. When some public health organization (or clueless MSM outlet) claims that an outbreak has been “controlled” by actions they have taken, the informed response is to question how much of this “control” was due to natural processes and how much of the “control” can be attributed to the intervention. Sometimes, the natural processes in play can even “mask” or hide harm from a “public health” intervention or policy. This is particularly true for many examples of common viral infectious diseases of childhood.
Most people who are not obsessed with viral infectious disease just notice local outbreaks. Perhaps when corporate media decides to launch another fear porn campaign for some reason, they might become aware of a regional outbreak within their country- such as the current “outbreak” of measles infection and disease occurring in Texas. They don’t notice that these outbreaks tend to periodically circle or spread across the world, strangely vanish for a few years, and then return.
Some background:
While the devil is in the details, and there is some seriously complicated mathematical modeling required to understand the nuances of outbreak timing (kinetics) and viral evolution during a spreading outbreak (cladistics) in specific situations, the general answer is mostly settled and can be understood without going too deep. But first, so that I can help bridge the gulf between academia and common knowledge, we need to define a very simple equation commonly used to describe how rapidly a virus will spread within a population - before it is even introduced. That equation defines the baseline infectivity of a virus in a specific population - the baseline coefficient of reproduction (R0).
If you were paying attention during COVID, you may have heard of this “coefficient of reproduction” - conveniently called R0 (R naught). R0 is so named because it describes, in an average way, how efficiently a virus will infect, reproduce and spread if nothing is done to slow it down. In a sense, this is a purely ‘academic” concept, but you have to start somewhere. In most cases, when an outbreak gets started, people at risk change their behavior, and some become infected right away and develop natural immunity (lets call this non-pharmaceutical interventions), and may start taking Vitamin D + Zinc, high dose Vitamin C, getting vaccinated (if available), etc. (lets call those things pharmaceutical interventions). These non-pharmaceutical and pharmaceutical interventions will make it harder for the virus to infect, reproduce and spread, and so will reduce R- let’s then call this a new “realistic” coefficient of reproduction R0’. At the start of an outbreak, R0 describes how many people (on average) will be infected by the first person(s) that have been infected. As soon as it starts infecting a population, people will get infected, recover, and develop natural immunity, and this process of acquiring “natural immunity” will start to slow the ability of the virus to spread- let’s call this moving target for the coefficient of reproduction Rn with n= the number of days (or weeks) after the virus enters the population and starts to spread. If either R0 (baseline) is greater than (>) 1 or Rn is >1, the virus will spread in the population.
If R0 or Rn is or becomes less than (<) 1, viral spread will slow and will quickly die out. In that case, each infected person will infect less than one other person, and the outbreak will be extinguished. Make sense? Simple stuff.
To predict the potential severity of outbreaks of infectious diseases such as SARS, HIV, TB and smallpox, a summary parameter, the basic reproduction number R0, is generally calculated from a population-level model. R0 specifies the average number of secondary infections caused by one infected individual during his/her entire infectious period at the start of an outbreak. R0 is used to assess the severity of the outbreak, as well as the strength of the medical and/or behavioral interventions necessary for control. Conventionally, it is assumed that if R0>1 the outbreak generates an epidemic, and if R0<1 the outbreak becomes extinct.
Herd Immunity
What about “herd immunity”? Remember Fauci making a series of public statements starting with ‘70- 75% vaccination” would lead to “herd immunity,” then he pushed it up to “80 - 85%”? All pretty much based on what he thought the American people would tolerate. Well, what this really revealed is that he was using technically impressive-sounding words that he either did not really understand or was lying to manipulate public opinion. Scientism.
Anthony Fauci is not actually trained in viral epidemiology. He just played a viral epidemiologist on TV. If he was what he was pretending to be, he would have understood the accepted general equation that describes the relationship between Ro and herd immunity. He would not have treated “herd immunity” as some sort of a seat of the pants estimate that he pulled out of a dark place. And, presuming that he can actually be professionally embarrassed, he would not have lied like this.
Herd immunity is the point at which Rn becomes less than 1 as a consequence of individual people acquiring “natural immunity,” in addition to the population-level effects of non-pharmaceutical and pharmaceutical interventions that the community-at-risk has implemented.
Those interventions can be universal (typically requiring mandates) or less than universal. All of these variables can be included in equations used to predict when “herd immunity” can be achieved - the equation just gets a bit more complicated but remains well within the competence of virtually any adequately trained epidemiologist. Which Anthony Fauci is not. He basically used the words of viral epidemiology without doing the actual work. Because he was spreading propaganda in an effort to manipulate the public for various reasons. He was not actually “doing science”.
Yet another example of how Fauci lies. Like a trained pro. Looking straight into the camera without blinking or other clear-cut “tell.” He must play a wicked poker hand.
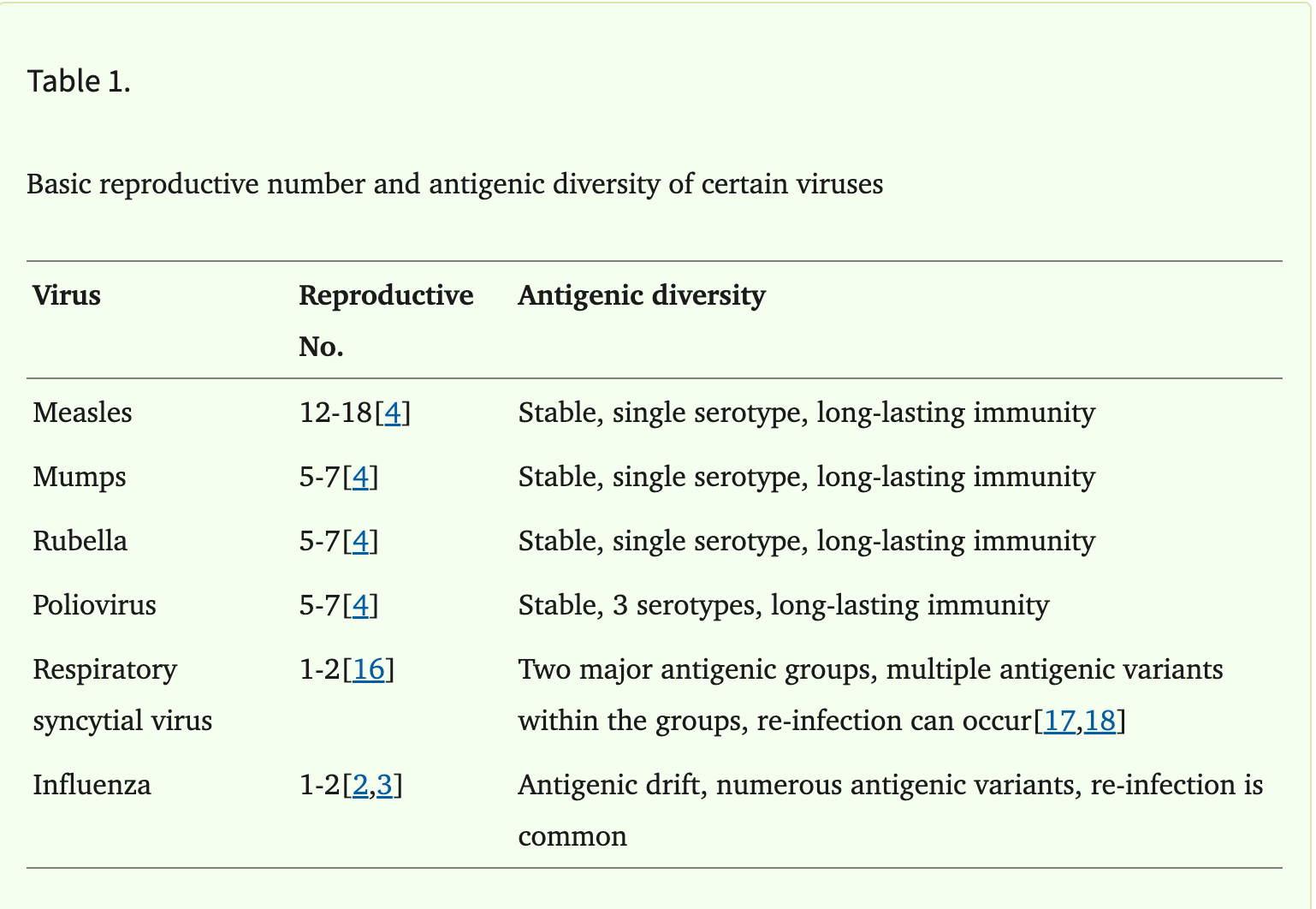
Pathogens with higher R0 require a higher herd immunity level. The baseline threshold herd immunity level for a specific virus and a specific population can be calculated by 1 - 1/R0. For example, a virus with R0 of 2 (each infected person on average will infect two other people) will achieve herd immunity level at 1 - 1/2 or when 50% of the population is protected from infection (more like influenza), whereas a disease with R0 of 10 (more like measles or COVID) will need a herd immunity level of 1 - 1/10 or 90% protection from infection.
Hence my notorious comment at the “stop the mandates” rally in DC where I said “the vaccine is not working, it is not preventing infection, replication or spread” for which some young clueless “journalist” from the Washington Post accused me (in print) of being a liar. But from a herd immunity point of view, which was how it was being (literally) marketed by Fauci and CDC to the public, this was and remains an absolutely true statement. Confronted by the now self-evident reality, the CDC and high priests of USG public health Scientism had to fall back on mumbling about how the vaccines reduced sickness and death - a debatable point which was not actually a measured outcome used by the FDA for the Emergency Use Authorization. But I digress.
In any case, are you still following this?
Now we can talk about what happens with an outbreak of a childhood infectious disease, and why (in the natural state) these larger waves of infectious viral outbreaks are seen in children for the most part.
If you take the long view, in the natural situation (no vaccines), most adults were infected by these “childhood infectious disease” agents (viral or bacterial) when they were young. They got the infection (think mumps, measles, chicken pox), recovered, and developed robust, typically lifelong immunity. Or are at least immune until their immune systems start to wear out - a process (not completely understood) called immunosenescence. In any case, in the historically normal situation most adults already have partial or complete natural immunity to virtually all of the “childhood” infectious diseases. Only the children have not been infected in the past. Why are these “childhood” infections?
When a virus gets introduced into a community, it tends to only spread in the subset of those that have not already been infected and recovered. As more and more children in that community become infected, recover, and develop natural immunity, it becomes increasingly difficult for the virus to spread from one child to another. In other words, the starting conditions that defined R0 have now changed. Let’s call this new condition Rn as described above.
What about the Children?
Of course, Rn will now be less than R0 because fewer children in the general population can be infected, so transmission is less efficient. As time goes by and more and more children are infected, recover, and develop natural immunity, eventually, the coefficient of reproduction drops below one - in other words, each infected child infects less than one other child (on average), and so the outbreak dies out. What an adult watching this observes (imagine an elementary school teacher surrounded by a concentrated group of children) is that the infectious wave starts, grows, and then slowly peters out. Seems like magic. And suppose some non-pharmaceutical (say masks and social distancing) or pharmaceutical (think school vaccine mandates) interventions have been imposed on those children. In that case, it is natural that our adult observer will conclude that these measures “worked,” when, in fact, most of what happened is most likely due to the gradual spread of natural immunity within the school kids.
In children, this tends to happen extra fast (relative to adults) because the anatomic part of their immune system that helps immunity to develop - called the thymus- is large and very active. But as we develop into adulthood, the thymus “involutes” or shrinks, and it’s ability to “educate” key immune cells to fight off infections decreases. So concentrated groups of vulnerable kids (school) often develop herd immunity faster than groups of vulnerable adults (think residents of eldercare facilities).
Hopefully, this explanation has made sense of the “wave” of infections that rises, peaks, and then “magically” falls off. Now, let’s discuss the basis of the loosely periodic nature of childhood infectious disease outbreaks. Here’s how that works, to a first approximation, using a real-world example.
Real World Example - Measles Outbreak in Texas
Imagine you have a socially cohesive group of people who are opposed to measles vaccination for some reason. Often, such groups are part of some intentional community that retains most of its member children into adulthood, and often, these communities are cohesive because of shared religious faith. However, there are many reasons that intentional communities develop. For now, please set aside any discussion of whether their opposition is rational. They just do not vaccinate their kids against measles.
Now, imagine that such a group is geographically located in Texas. An area under pressure from unvaccinated immigrants coming across the southern border who are arriving from regions of the world that do not typically vaccinate against measles - due to poverty or public policy, the reason is irrelevant. Within some subset of these immigrants, will be those that are either acutely sick with measles, about to develop measles (pre-clinical infection) or harbor latent measles virus for some reason. Imagine that these immigrants introduce measles virus into the part of Texas where this intentional community with unvaccinated children have been doing just fine up until now.
In other words, this intentional community of Texans has not been exposed to measles for many years, therefore for years has not had an opportunity to develop “natural immunity” and has also not been exposed to a partially effective measles vaccine that is more protective than nothing, but less protective than natural immunity.
In this case, the measles virus will spread very rapidly within this intentional community. It will spread until Rn becomes less than 1 as a consequence of individual people acquiring “natural immunity,” or accepting the (previously avoided) vaccine. A wave of infection. And if the surrounding population of Texas that are in occasional contact with the members of this community have been treated with a less-than-perfect vaccine, some fraction of those “vaccinated outsiders” will also become infected. And all vaccines are less than perfect at protection. Whether the measles vaccine is 97% protective against infection (for an “average” infectious dose) or 50% protective, SOME fraction of the surrounding Texas population will get infected.
Eventually, Rn becomes less than 1 in both the theoretical “intentional community” and the surrounding population of vaccinated Texans. “Magically,” the wave of measles infection is quenched. Whether or not the vaccine-resistant community starts accepting measles vaccine.
But then, the members of this intentional community have children. Year after year, and gradually, more and more unvaccinated children from each age cohort build up. And some of the elders develop immunosenescence and they also become at risk for measles infection. At some point, the average resistance of the community (as a population) drops to the point that if a measles virus is again introduced in some random event, another wave of infection develops in that community, and the cycle repeats itself in a generally periodic fashion. And what an astute observer sees is a “childhood infectious disease,” because the majority of members of the group that have not previously developed “immunity” (natural or otherwise) are children. Furthermore, the more time elapsed since the last “wave” of infection, the more severe the next outbreak. And from this you can see how the logic of “measles parties” or “chickenpox parties” makes sense. Kids generally get less severe disease than adults (remember the thymus?), and so it makes sense to quite literally protect the elders by helping the children quickly develop “natural immunity” as soon as possible. This strategy can also help prevent “big” outbreaks by keeping the group of community members that have not developed “natural immunity” as small as possible.
Now scale this up.
Instead of an “intentional community,” think of a nation-state with relatively secure borders or geographic region separated from neighbors by a mountain range (Switzerland, the Romanian Transvall, Tibet etc.) Same dynamics, larger scale. The region does not vaccinate for measles, for whatever reason. Now imagine tourists traveling into that region. At some point, some tourist or immigrant will introduce measles virus into the region, it will sweep through the population in a wave, and then will die out as “natural immunity” becomes the norm. And then children are born, year after year, and at some random point some tourist or immigrant introduces measles virus into the region, and it’s off to the races.
If you are a viral epidemiologist monitoring this process, what you will observe is semi-periodic waves of childhood infectious diseases sweeping across the world. But it all comes down to birth cohort size, timing, travel, and R0, the average number of secondary infections caused by one infected individual during his/her entire infectious period at the start of an outbreak.
There. If you have been following along, now you know more about viral epidemiology than Anthony Fauci does.
Hopefully, if you have been able to follow this, you now have a better understanding of what is going on with measles in Texas (and Ontario, Canada, the European region, and the entire world) at this point in time.
Advanced Topic: Why do Viruses with High Reproduction Numbers tend to be genetically stable, and Viruses with Low Reproduction Numbers tend to evolve rapidly?
This is an interesting question, and current thinking may need to be revised based on what has happened during COVID, where the SARS-CoV-2 virus evolved from having a lower reproduction number (closer to seasonal influenza) to a higher reproduction number (closer to measles).
As I was reviewing recent literature to make sure that my understanding of these issues relating to infection waves and viral epidemiology was still current, I ran into a very interesting paper that addresses this question. Some of you may enjoy reading it and responding with your own thoughts and criticism.
Link here- Viral evolution and transmission effectiveness
Abstract
Different viruses transmit among hosts with different degrees of efficiency. A basic reproductive number (R0) indicates an average number of cases getting infected from a single infected case. R0 can vary widely from a little over 1 to more than 10. Low R0 is usually found among rapidly evolving viruses that are often under a strong positive selection pressure, while high R0 is often found among viruses that are highly stable. The reason for the difference between antigenically diverse viruses with low R0, such as influenza A virus, and antigenically stable viruses with high R0, such as measles virus, is not clear and has been a subject of great interest. Optimization of transmissibility fitness considering intra-host dynamics and inter-host transmissibility was shown to result in strategies for tradeoff between transmissibility and diversity. The nature of transmission, targeting either a naïve children population or an adult population with partial immunity, has been proposed as a contributing factor for the difference in the strategies used by the two groups of viruses. The R0 determines the levels of threshold heard immunity. Lower R0 requires lower herd immunity to terminate an outbreak. Therefore, it can be assumed that the outbreak saturation can be reached more readily when the R0 is low. In addition, one may assume that when the outbreak saturation is reached, herd immunity may provide a strong positive selection pressure that could possibly result in an occurrence of escape mutants. Studies of these hypotheses will give us an important insight into viral evolution. This review discusses the above hypotheses as well as some possible mechanistic explanation for the difference in transmission efficiency of viruses.











RFK’s Jr’s recent statement about continuing with the measles vaccine in Texas begs the question of is he right? Or should he be explaining the information put forth in this article, or both? I, over the years past 70, have refused my doc’s urging to get the shingles shot. My neighbor gets it and has had three extreme episodes of the virus. I did get it but all that happened was the rash and itching. Never any pain as people seem to experience. Did let the doc talk me into the pneumonia shot 14 years ago and I came down with it. So I don’t put much stock in some of these ‘preventative’ vaccines. At 88 I’ll stick to my higher doses of Vit C and D, a couple other supplements and nasal flushing. Still live in a single residence and plan to live this way til death.
So informative! Always looking after your fellow Americans. Helping to keep us free and informed. So appreciate you and your wife for staying in the fight. ❤️🌹