



More Important Ivermectin Study Results
Plus- prescribing drugs "off label' is important, and the "emergency" is over

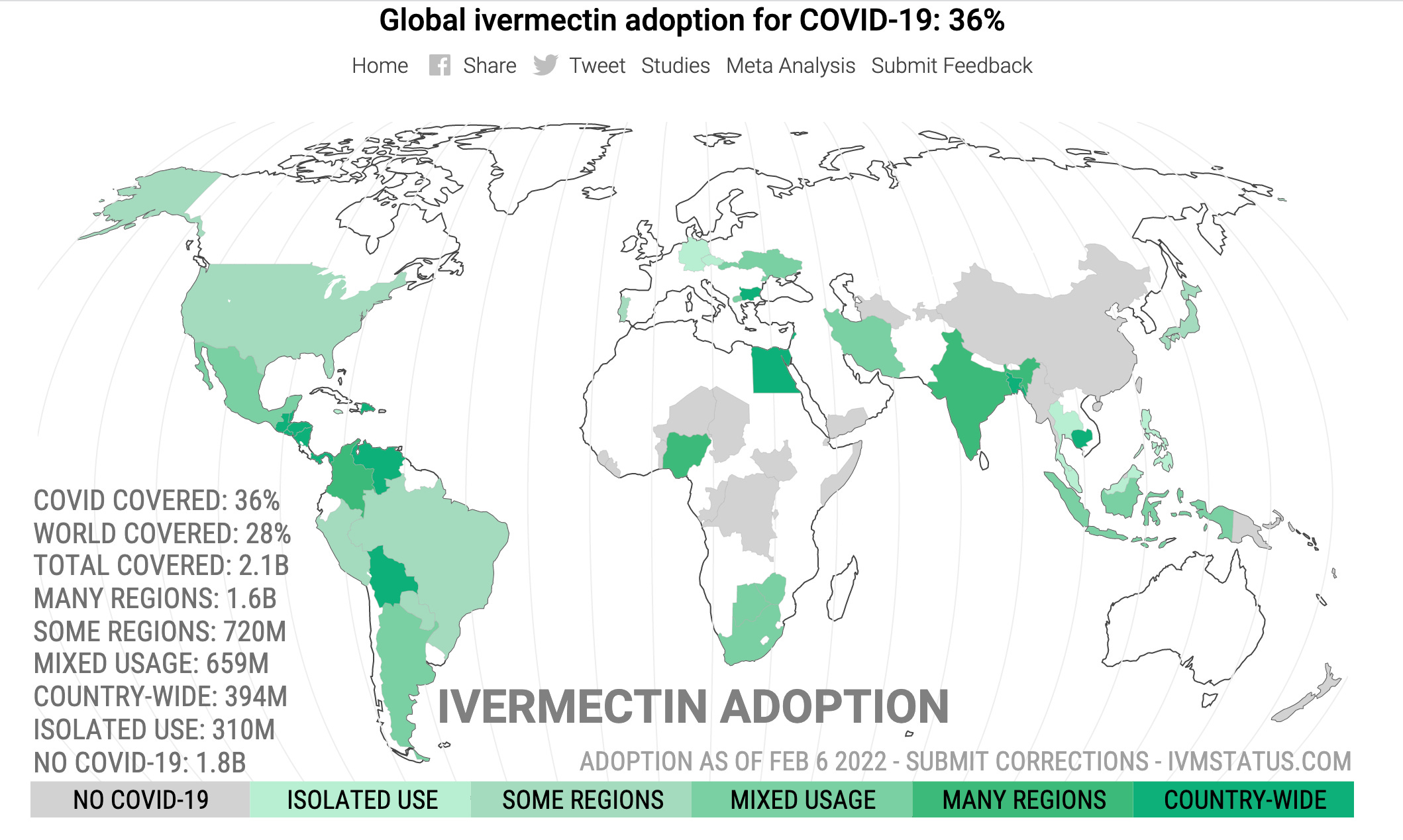
Click here for more details on the map above
Strictly regular use of ivermectin as prophylaxis for COVID-19 leads to a 90% reduction in COVID-19 mortality rate, in a dose-response manner: definitive results of a prospective observational study of a strictly controlled 223,128 population from a city-wide program in Southern Brazil
Research Gate, February 2022 DOI:10.13140/RG.2.2.20069.68320
This important preprint needs to hit alternative and mainstream media now.
The Study:
Background: Previously, we demonstrated that ivermectin use as prophylaxis for COVID-19 was associated with reductions in COVID-19 infection, hospitalization, and mortality rates, and in the risk of dying from COVID-19, irrespective of regularity and accumulated use of ivermectin, in an observational, prospectively obtained data from a strictly controlled city-wide program in a city in Southern Brazil (Itajaí, SC, Brazil) of of medically-based, optional use of ivermectin as prophylaxis for COVID-19.
In this study, our objective was to explore the data obtained from the program to evaluate whether the level of regularity of ivermectin use impacted in the reductions in these outcomes, aiming to determine if ivermectin showed a progressive dose-, regularity-response in terms of protection from COVID-19 and COVID-19 related outcomes.
Materials and methods: This is a prospective observational study of the program mention above, that used ivermectin at a dose of 0.2mg/kg/day for two consecutive days, every 15 days. We obtained and analyzed the data regarding the accumulated dose of ivermectin use, in addition to age and co-morbidities, to analyze the patterns of reduction of COVID-19 infection, hospitalization, and mortality rates, and risk of dying from COVID-19, according to the regularity and amount of ivermectin used in a 5-month period.
Following definitions of regularity, we considered as strictly regular subjects that used at least 180mg of ivermectin (180mg = 30 tablets), and as sporadic users subjects that used 60mg (= 10 tablets) or less during the 5-month period.
Comparisons between subjects that did not use ivermectin and these two levels of regularity of ivermectin use were performed. Analysis of the intermediate levels of ivermectin use are present in the supplement appendix of this study. To analyze hospitalization and mortality rates, we utilized the database of COVID-19 infections of all participants, from Itajaí and outside. To analyze COVID-19 infection rate and risk of dying from COVID-19 we utilized the Itajaí city database.
Propensity score matching (PSM) was employed, followed by multivariate adjusted analysis for residual differences (doubly adjusted analysis).
Results:
Of the 7,345 cases of COVID-19, 3,034 occurred in non-users, 1,627 in sporadic users, and 289 in strict users, while the remaining cases occurred in the intermediate levels of ivermectin use. Strict users were older (p < 0.0001) and non-significant higher prevalence of type 2 diabetes and hypertension.
COVID-19 infection rate was 39% lower among strict users [4.03% infection rate; ( p < 0.0001] than in non-users (6.64% infection rate), and non-significant 11% reduction compared to sporadic users (4.54% infection rate) (n = 1,627 in each group; RR, 0.89; 95%CI 0.76 – 1.03; p = 0.11).
Hospitalization rate was reduced by 100% in strict users, compared to non-users and to sporadic users, both before and after Propensity score matching ( p < 0.0001).
After Propensity score matching, hospitalization rate was 35% lower among sporadic users than non-users (RR, 0.65; 95%CI, 0.44 – 0.70; p = 0.03).
In propensity score matched groups, multivariate-adjusted mortality rate was 90% lower in strict users compared to non-users (p = 0.003) and 79% lower than in sporadic users (p = 0.05), while sporadic users had a 37% reduction in mortality rate compared to non-users (p = 0.043).
Risk of dying from COVID-19 was 86% lower among strict users than non-users (p = 0.006) and marginally significant, 72% lower than sporadic users (p = 0.083), while sporadic users had a 51% reduction compared to non-users (p = 0.001).
Conclusion: Non-use of ivermectin was associated with a 10-times increase in mortality risk and 7-times increased risk of dying from COVID-19, compared to strictly regular use of ivermectin in a prospectively collected, strictly controlled population.
A progressive dose-response pattern was observed between level of ivermectin use and level of protection from COVID-19 related outcomes and consistent across different levels of ivermectin use.
The results of this study clearly demonstrate that prophylactic use of ivermectin must be initiated immediately for people in high risk categories in the United States and worldwide. This includes individuals with one or more co-morbidities and the middle aged/elderly. Our “design-to-fail” government funded clinical trials for early treatment and governmental obstructionism regarding life saving treatments to patients must end now.
The CDC chart below for all deaths since the start of the outbreak clearly shows a jump in deaths after 50 years old.
However, as the data for deaths per million per age group is not disclosed, so the age for start of prophylaxis has yet to be determined.
As Omicron has less pathogenicity and slightly different disease profile this too could influence what age prophylaxis treatment should begin. But the data are in, prophylactic use of ivermectin saves lives.
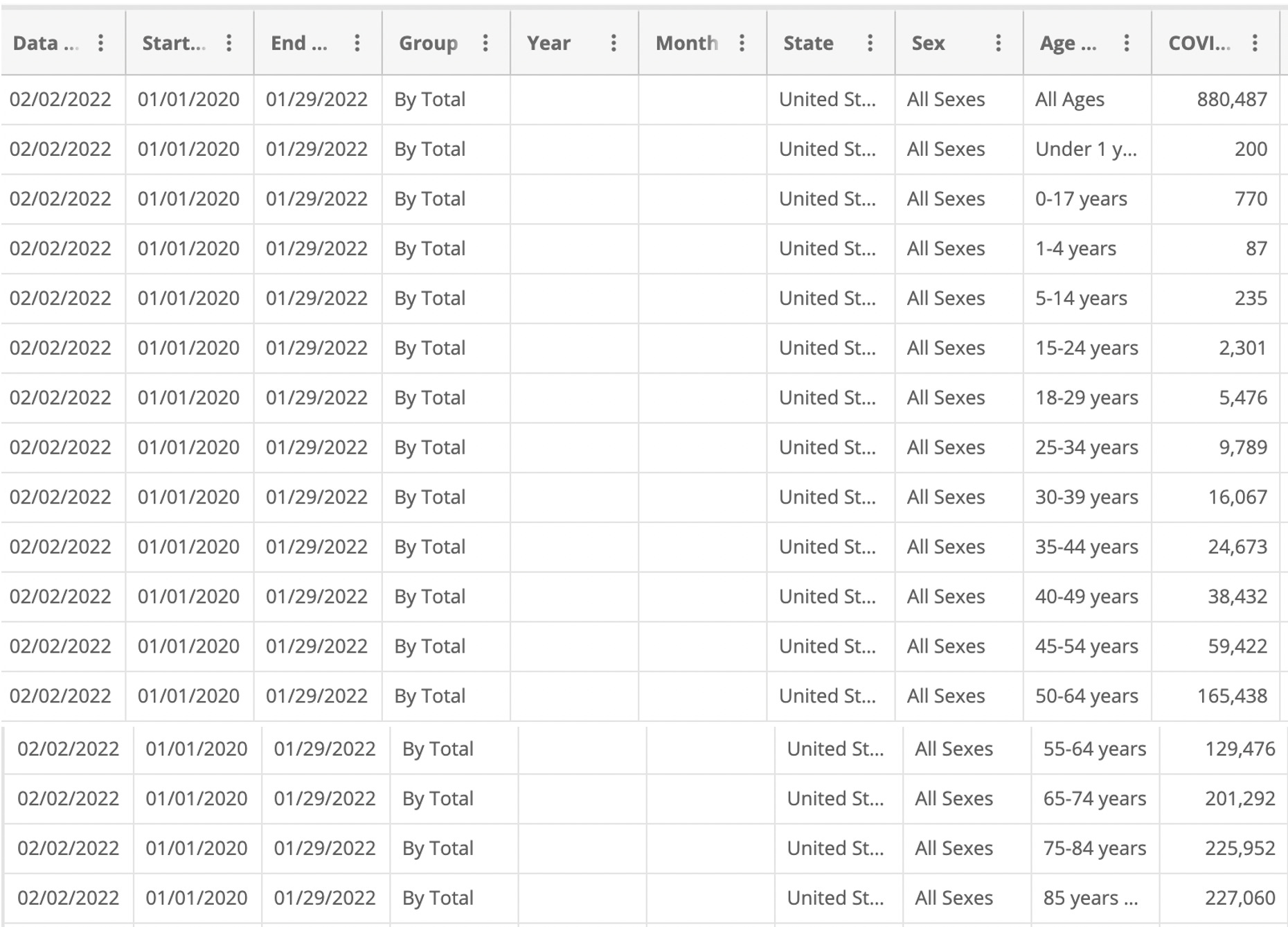
In regards to the table above, the age stratification of disease shows why a universal vaccination program for a vaccine with a high adverse event profile is not advised. It is time to stop all mandates at the Federal and State level. It is time to stop pushing this vaccine on children.
Research and clinical practice show that using re-purposed drugs for Covid-19 have huge benefits. These include multi-drug, multi-staged treatments for Covid-19 disease that prevent severe disease, decreases hospitalization rates and decreases death. It is time our government and state licensing board recognize this and let physicians practice medicine.
'Off-label' drug use: an FDA regulatory term, not a negative implication of its medical use. Int J Impot Res. 2008 Mar-Apr;20(2):135-44. doi: 10.1038/sj.ijir.3901619. Epub 2007 Nov 15. PMID: 18004389.
Highlights:
A doctor's decision to inform the patient of the 'off-label' status of the prescription is not relevant to the physician's standard of care for an informed consent case.
The FDA has specifically stated that its procedures and requirements have no effect on the practice of medicine and that the FDA does not prohibit doctors from prescribing drugs in an 'off-label' manner.
The FDA's approval of a drug is immaterial to the effectiveness in the drug's 'off-label' use. In fact, prescribing medication in an 'off-label' manner can constitute the standard of care in many cases.
A doctor's duty is to practice medicine and treat his patient, not inform the patient of the FDA's non-medically related labeling. Therefore, doctors should not be branded with the additional duty of disclosing non-pertinent information, such as the FDA's medically irrelevant distinction, to their patients
*It is estimated that 21% of all prescription drugs are prescribed “off-label.”
For fun, I took the countries that reportedly use Ivermectin country-wide and compared them to the USA, Israel and Sweden. I chose a three month cut-off, although the results were extended further. I did this because I don’t know when some of the countries began ivermectin use.
Can you guess who now has the highest death rates per million? Yeh -
USA
Israel
Sweden
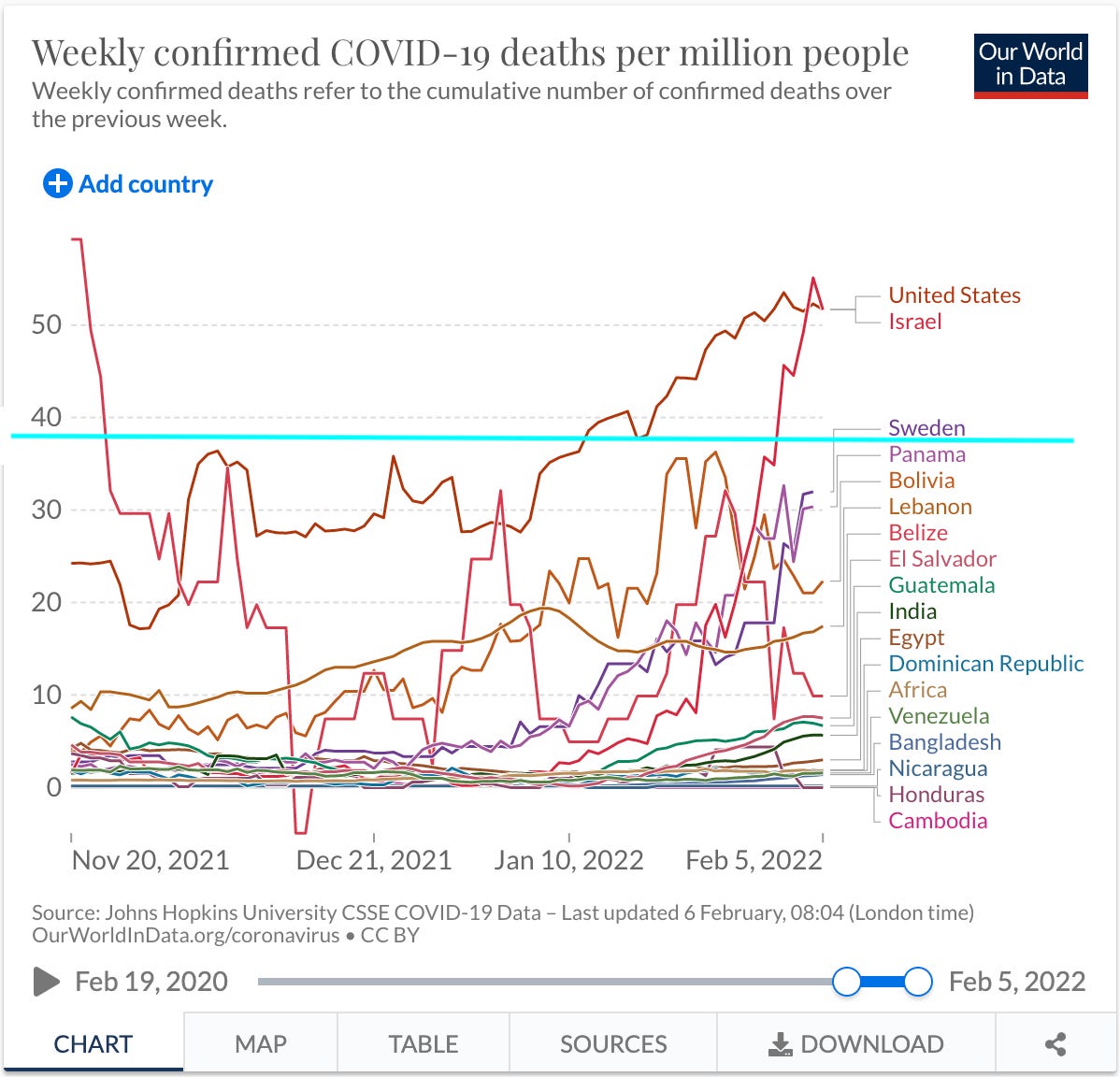
Notes: I included - India, because although not all regions use Ivermectin - although the most populated due. Likewise Africa - which many nations treat with ivermectin prophylactically and these world maps do not break down Africa by Nations (weirdly imperialistic). I did not include Bulgaria, as although they use ivermectin - their death rate numbers are skewed for other reasons not worth delving into.
There are a lot of confounding variables here. Such as natural immunity, vaccination rates of the elderly and those with co-morbidities, as well as seasonality of the virus, vitamin D3/zinc levels and age of population.
But it is still an interesting snap shot as to where much of the world is right now.








I cited that disinformation-crushing Brazil study in a recent conversation I had with a pharmacist. I shared this story at a recent Steve Kirsch post, but I think it bears repeating here as it’s something anyone can do to start red-pilling key figures.
I had gotten a prescription for IVM from an FLCCC provider (https://covid19criticalcare.com/ivermectin-in-covid-19/covid-19-care-providers/), and I had them call it into my standard mail-order pharmacy. They said they couldn’t fill it because they don’t do compound meds, but they forwarded me to the pharmacist to discuss the details.
I spontaneously decided to ask the pharmacist what he thought about ivermectin as part of an early treatment protocol for COVID. He stammered out a few propaganda talking points, such as studies about IVM being dangerous in high doses and that you have to take high doses for it to be effective. I asked if he’d heard about the recent Brazil study demonstrating its effectiveness in a population of 223,000. I mentioned its record of efficacy in Uttar Pradesh, Africa, and Japan. I asked if he was aware that it had a 40-year track record of safety and had been shown by numerous peer-reviewed studies to be highly effective against COVID. When he mentioned hearing things about ivermectin on the news, I mentioned that that was disinformation propaganda being funded by pharmaceutical corporations because having people know there is a safe, cheap, and effective medication available for treating COVID threatens their billion-dollar vaccine profits.
He mentioned that he generally follows information from the CDC, and I asked him if he knew what regulatory capture was. He did not. I then said if I can plant one seed to please read "The Real Anthony Fauci" to understand the degree of the corruption, propaganda, and disinformation coming from the pharmaceutical industry and allied agencies.
The pharmacist seemed genuinely interested and said he was going to look into it that afternoon. Asking a few simple questions, planting the seeds of doubt, and pointing him to some studies and the RFK Jr. book appeared to have had an impact on his attitude toward ivermectin and the larger corruption the coverup about its efficacy pointed to.
If we can engage in simple conversations like this with everyday people who are solely being exposed to propaganda—especially those in the health care industry—we may be able to have a ripple effect across the world population.
The only News commentators that will share this are, Jesse Waters, Tucker Carlson and Laura Ingram.