
Vaccines and the Length of Our Lives
Calculating risk versus benefit


By David Bell
The commercial imperative to extract money from human bodies is playing havoc with medical education, and the body of knowledge through which the medical professions operate. Nowhere is this more apparent than in the field of vaccines, and their place in determining the length of our lives.
The History of Living Longer
As a medical student, I was taught that the reason we in wealthy countries now live far longer than our forebears was improvements in living conditions, sanitation, and nutrition. We don’t walk through sewage and horse dung each day, eat fly-blown meat, drink water from below the nearest latrines, or sleep eight to a room on rancid bedding. We get beaten less often and have more leisure time. Antibiotics also helped but came after most of these gains had been achieved.
Most vaccination came even later, mopping up some residual mortality in ‘vaccine-preventable diseases.’ This was all stated in a lecture hall of 300 medical students, with the relevant data to back it up, and accepted as fact. Because for wealthier countries it was, and is, undeniably true.
I recently asked a small group of students the major reasons for improved life expectancy, and was told “vaccination.” In a subsequent session, I showed some of the graphs laid out below. The students were shocked and asked where I obtained this information. It was actually fairly difficult to find. I remember searching 20 years ago and readily finding it on the web.
In 2024, it took a lot of sifting through information explaining how vaccinations have apparently saved humanity, and how those repeating what I was taught as a student were a subversive element undermining the greater good, spreading misinformation or similar daft claims. We have certainly not progressed.
This does not mean vaccines are not a great idea. Providing some immunity before an infection can mitigate much of its harm by giving the body a head start in fighting back. It just means their usefulness must be understood in context, as must their harms. Somewhat strangely, discussion of vaccines has become increasingly controversial within the medical establishment. It is as if an Inquisition has been imposed over the profession, seeking out anyone still prioritizing calm rational thought over a dogma dictated from above. However, if truth and calm discussion can form an anchor for policy, vaccination will be more effective.
The charts shown here, from Australia, the United States, and England, reflect those of other wealthy countries. The same findings are reflected in various published papers. Facts are facts, even if they may with time become harder to find, buried under Big Search algorithms to keep us safe. They remain facts even if medical students are taught to believe alternate realities. Such false teaching, coupled with large financial incentives, drive their desire to ensure children be ‘fully vaccinated’ according to their country’s childhood schedule. They increasingly believe a lie, undeniable misinformation, that this is why most children in our countries now grow up without experiencing the death of a friend or sibling.
Vaccines in Context
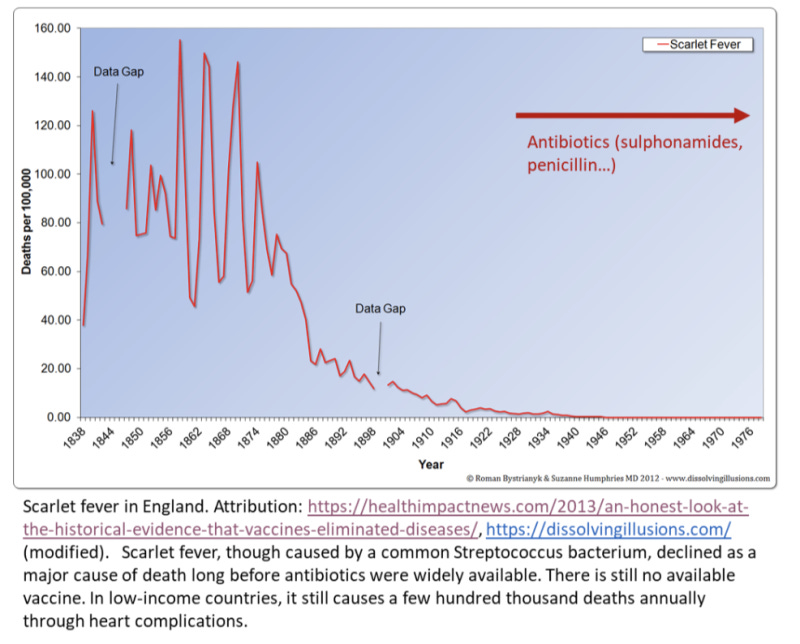
The medical world calls these “vaccine-preventable diseases” because companies sell vaccines that can prevent them. They are vaccine-preventable to a large extent, and vaccines do stop them from killing people. But in wealthy countries, truthfully, the numbers they save are very low.
Vaccination probably had a major role in the elimination of smallpox. We cannot, of course, be absolutely sure, as there was no control group. Smallpox caused outbreaks that decimated populations isolated for thousands of years from the virus, such as Native Americans, where a vaccine would have made a massive difference.
However, smallpox also had the hallmarks of a disease that might actually disappear through good public health education and improved living standards; it lacked an animal reservoir, required close contact with body fluids to spread, and was usually easy to recognize. It is probable that the vaccine considerably accelerated its decline, especially in poorer countries.
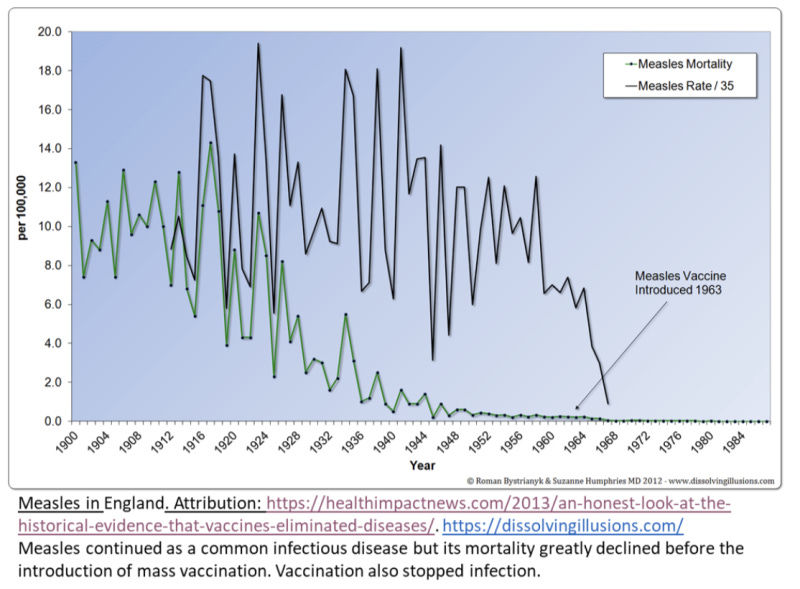
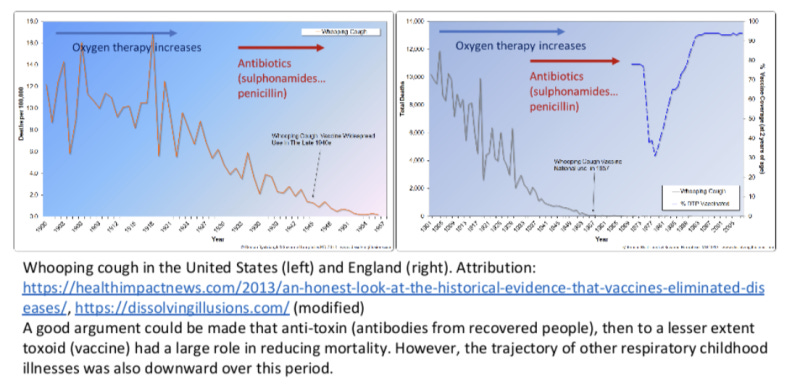
Measles is similarly interesting. As the graphic shows, most decline was long before mass vaccination. Like whooping cough, mortality was probably partly reduced through the advent of oxygen therapy, but mainly people just appear to have become less susceptible to its complications.
It could nonetheless be a devastating disease, which decimated isolated, immunologically-naïve populations in the Pacific Islands and elsewhere that had no history of contact, and still causes avoidable child death in low-income countries today. Measles deaths are often associated with micronutrient malnutrition, such as vitamin A deficiency, and fixing that would also address many other health risks. This used to be emphasized 30 years ago.
However, the measles vaccine is also very effective at stopping measles deaths in susceptible populations. It has very little impact on mortality in wealthy countries where it mainly stops infection and annoying sickness, as few kids are so micronutrient-deficient to be susceptible to very severe diseases. It is so good at stopping actual infection that mandates for measles vaccines that some countries impose are more about authoritarianism than public health.
If you don’t want your child to risk measles and decide that vaccination is a lesser risk, you can have your child vaccinated. Your child is now protected from those who are unvaccinated, so there should be no interest in mandating it for them. Rational free people could live with that.
Hepatitis B and HPV vaccination (for Human Papilloma Virus) are two further curiosities. We schedule Hep B vaccination on the first day of life, even though it is mainly spread in Western countries through sexual contact and intravenous drug use. If the parents are not infected (and all mothers are screened), then there is not really a risk until the late teenage years, when the person can make their own informed choice. For a child born in a country with 30% Hepatitis B positivity rates and poor healthcare, the risk-benefit calculation may produce a different result. Dying of liver failure or liver cancer is not pleasant.
The HPV vaccine, intended to prevent cervical cancer, has a complicated picture. It will have limited mortality impact in Western countries where cervical cancer mortality has already declined through regular screening. Elsewhere the situation is very different, with over 300,000 women dying annually from this agonizing disease, mostly in regions such as sub-Saharan Africa where only about 12% are screened. This is not through choice but because screening is poorly accessible. As development of cancer can take about 20 years after HPV infection, we must also rely on (reasonable) assumptions about causality when calculating benefits. So, the equation clearly varies between women.
Calculating risk versus benefit in order to ensure clear informed consent (or even medical ethical competency) would require consideration of age, behavior, access to screening, and adverse event rates. To know adverse event rates, a comparison would logically be necessary between the vaccine and something neutral like saline (rather than other vaccine constituents). Because this is still awaited, women should of course be informed of this data gap. Therefore, a blanket policy on HPV vaccination would be illogical.
The story of diphtheria suggests that medical management may have had a major role in its decline. The decline coincided with the introduction of antibody therapy (anti-toxin), and later decline with the toxoid vaccine. However, it also coincided with the decline of other respiratory diseases of childhood that did not have such interventions. So, we simply cannot be sure.
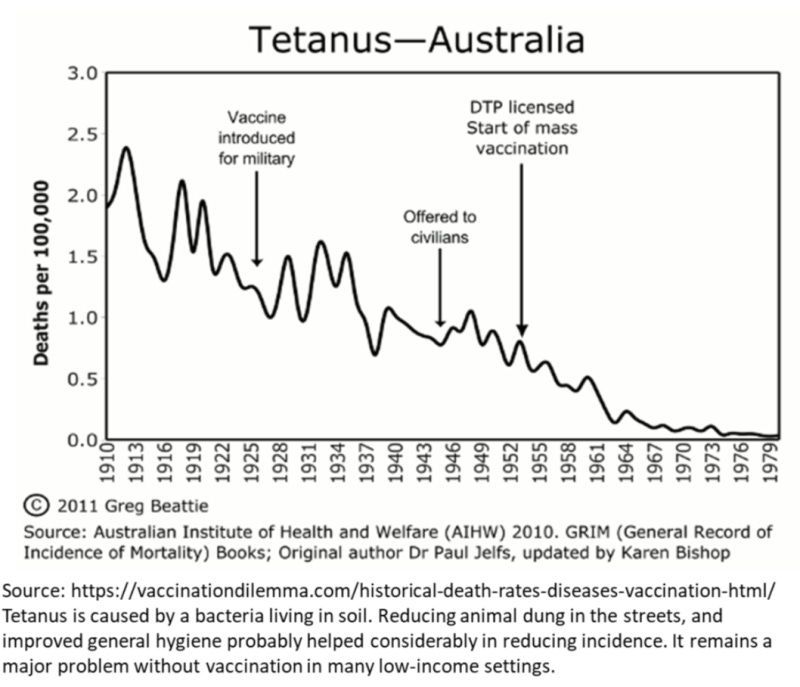
Tetanus toxoid may also have had an impact, especially for people at higher risk, such as plumbers and farmers. However, accountants no longer navigate dung-paved streets on the way to the office and this general cleaning up of the environment will have driven much of the change. For business reasons that are slightly unclear, boosters are available only combined with diphtheria and pertussis vaccines in many Western countries, which adds nothing to an adult’s benefit but adds to their risk. It’s hard to claim safety and benefit are the main drivers in the face of such an anomaly.

Knowing What We Don’t Know
All vaccines also have adverse effects. While not discussed here, they are real and I know people whose health was wrecked by vaccination. Assessment of risk is difficult as no childhood vaccines on the US schedule have been through a true placebo-controlled trial – they are usually compared against the rest of the contents of the vial (chemicals such as adjuvants and preservatives but lacking the antigen or inactivated virus – a mixture that may be the cause of most of the side effects) or against another vaccine.
By doing this, they can be shown to be no worse than the comparator, which would be fine if we actually had decent placebo-controlled trials of the comparators. Most doctors who prescribe vaccines almost certainly don’t know this. (There is a good, evidence-based explanation of this issue which is well worth reading).
Most doctors probably also pay little attention to the lack of trials determining the effect of giving dozens of doses of immune-stimulating adjuvants and preservatives, including aluminum salts, to growing children across their formative years. It is likely to be relatively harmless to many children, but harmful to some, as biology tends to work that way. However, if the disease that it addresses is hardly ever severe, then that ‘some’ can become very significant. Each ‘some’ is a child whose parents are trying to do the right thing, and trusting the medical establishment that this is indeed being done.
None of this would be new to a lot of people, as interest in vaccines and their harms and benefits is growing. However, most doctors performing vaccinations are probably unaware of much of the above, especially those graduating in the past couple of decades. If they are aware, they will likely be scared to discuss it as this would risk being labeled a “vaccine denier” or similarly childish term, or seen as promoting “vaccine hesitancy.” Vaccine hesitancy is what we once referred to as informed consent (or thinking before doing). After World War Two, we decided that informed consent was essential for ethical medicine. Now, the World Health Organization considers such independent thought a particularly dangerous threat to their interests and those of their sponsors.
Many recently trained doctors would consider the lecture I attended 40 years ago a public health risk, and the facts we were shown ‘misinformation.’ They will, at least in the US, also graduate with massive debt and be quite dependent on the subsidies they can receive from medical insurers, which include offering or giving vaccinations. This is why they can be so dismissive of intelligent people who spend time reading up on, and questioning, such things. They are not being aggressive or intentionally batting for Big Pharma; they are just so indoctrinated in the selling of these health commodities, and so financially and professionally dependent on this being the best course, that they are unable to articulate an independent, rational, evidence-based stance.
Navigating a Rational Path
To understand the vaccination issue, the public needs to understand that the medical and public health professions have lost their ability to reason. They are experts in repeating what they were taught, but not in deciphering reality. There are also fanatics and dogmatic people on the other side of the vaccine divide that can see the harms, but not the good.
They downplay a few hundred thousand cervical cancer deaths per year, and have not witnessed the gut-wrenching sight of a baby dying of tetanus in a low-income country with no ability to address her pain. They have not had to send a rabies sufferer home to die because there is simply nothing the local medical system can do for them once they are symptomatic.
On vaccination policy, the public mostly needs to go it alone. Understand there are real risks and real benefits, like any pharmaceutical. Understand that the main reason why we don’t die from many of the infectious diseases that we used to has little to do with vaccination. Listen to a doctor, then ask them some pointed questions to ascertain whether they are looking at your child in context and weighing both sides or simply reciting a script.
When the benefits clearly outweigh the risks, vaccines make sense. They are a foolish idea when the opposite applies. It’s difficult to navigate the information out there, but the public must do so until the medical establishment frees itself from the shackles of its sponsors and catches up.
Everyone should be hesitant to have stuff injected into them for commercial profit. We should hesitate more when the person injecting it is also rewarded for their compliance. Doctors should be hesitant about injecting chemicals and metal salts into anyone unless they have strong expectations of net benefit. With vaccines, as with antibiotics and almost any other pharmaceutical, sometimes they will have and sometimes they won’t.
Obviously, governments should not be mandating the injection of commercial chemicals as a requirement to participate in society – that would be ridiculous. A State can never make such individual cost-benefit assessments, and in a democracy, we certainly don’t pay the government to own and direct our bodies.
This is all so obvious, and inline with conventional evidence-based practice, that you really wonder what all the fuss is about.
This article was first published at Brownstone Institute.
Dr. David Bell, is a Senior Scholar at Brownstone Institute and is a public health physician and biotech consultant in global health. David is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
When I went to UC Berkeley's School of Public Health back in the late 1970s, we were taught that the primary reason that America "conquered" the various epidemics was NOT due to a medical treatment or any vaccination, but it was due to various public health efforts (improving water supplies, better sewage treatments, and access to a greater variety of foods).
We were also taught that the primary reason that people were living longer was again NOT the result of medical treatment, but it was because infant deaths (from zero to 5 years of age) declined. Further, if a person was 40 years old in 1900 and another person was 40 years old in 1960, they had almost the same chance of living until 70 years of age.
Nowadays, people are mis-taught that vaccination had a "major" effect on longevity.
This misinformation is due to the schools of public health that are getting increased amount of grant money from Big Pharma companies.
This kind of information is so important because vaccines have been given God like status but their importance is relatively minor and that doesn't take harms into account. Many of them have net negative value.